NSW public hospitals are spending roughly 70% of nurse and doctor time on administrative work — not patient care. At the same time, a national healthcare worker shortage exceeding 600,000 people is making every clinical hour harder to find and more expensive to replace. The administrative burden is not a cultural problem or a staffing problem. It is an automation problem, and the tools to solve it are already deployed in Australian health settings.
Hospitals like Westmead, Prince of Wales, and John Hunter are operating under conditions that make the status quo unsustainable. Document volumes have surged by 305% in some settings, discharge coordination consumes specialist time, and emergency departments are triaging patients at the front door the same way they did two decades ago. The result: delayed discharges, spiking overtime costs, and clinicians who trained to treat patients spending their shifts processing paperwork.
What has changed is the accessibility of AI systems capable of handling these tasks. A NSW private hospital documented $670,000 in annual savings — reducing per-document processing costs from $2.80 to $0.50 — after deploying AI document automation. That figure reflects a 12-18 month engagement, not a multi-year transformation programme. The skills gap that once made this kind of deployment impossible for most health organisations is now bridgeable through external delivery contracts that handle the entire build and rollout.
This article examines the three AI applications delivering the clearest return for NSW health operations in 2026, the benchmarks that support them, and a practical 6-phase framework for organisations that want to start without building an internal data science team.
What You'll Learn
- Why AI adoption in healthcare is accelerating in NSW in 2026
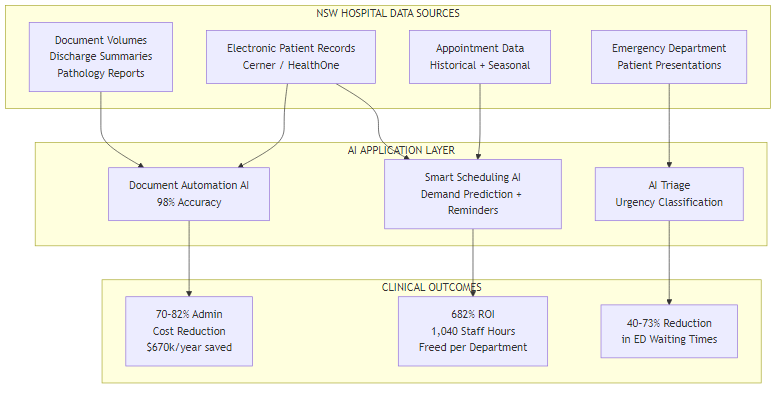
- How AI document automation is cutting processing time from 10 minutes to 3 — with 98% accuracy
- Why smart scheduling delivers 682% ROI and frees over 1,000 staff hours per department annually
- How AI triage systems are reducing emergency department waiting times by 40–73%
- A practical 6-phase implementation framework built for organisations without in-house AI teams
- Where to start if your hospital has no data science capability today
Reading time: ~8 minutes | Decision time: 30 minutes to identify your starting point
Why AI Is Now Accessible for Healthcare Organisations
For most of the last decade, AI in healthcare meant academic research, regulatory pilots, or large-scale deployments at the type of institution that could afford a dedicated innovation unit. The barrier was not the technology. It was the cost and complexity of connecting AI systems to clinical workflows, ensuring data privacy compliance, and sustaining the specialised team required to keep those systems running.
Those barriers have not disappeared — but they have shifted. Pre-trained document processing models now arrive with healthcare-specific fine-tuning. Integration with major EPR platforms like Cerner and HealthOne has become a known pathway rather than a bespoke engineering challenge. AHPRA-compliant governance frameworks have been developed and tested across multiple deployments. The practical result is that an organisation willing to engage an external delivery partner can move from assessment to a live system in as little as four weeks for targeted use cases.
Similar conditions exist in Queensland and Victoria, where health networks are exploring the same three application areas. But the NSW context — with its concentration of major public hospital campuses and a demonstrated appetite for digital health initiatives through the NSW Agency for Clinical Innovation — makes it a natural environment for accelerated adoption. The benchmarks reported here come from Australian deployments, not overseas projections.
Win 1: Admin Automation — Cutting Document Processing by 70–82%
The Problem
Administrative document handling — including discharge summaries, pathology reports, referral letters, and consent forms — has grown faster than staffing capacity can absorb. In some NSW health settings, unhandled document volumes have increased by 305% while workforce headcount has remained flat or declined. A document that takes a clinician or administrator 10 minutes to manually classify, extract, and route represents a meaningful draw on time that cannot be recovered from patient care.
A NSW private hospital reduced document processing costs from $2.80 to $0.50 per document after AI deployment — saving $670,000 annually — while handling a 305% surge in volume without adding staff.
The AI Solution
AI document processing systems use optical character recognition combined with natural language models to scan, classify, extract, and route documents with accuracy rates of 98% or above. The processing time per document drops from roughly 10 minutes to 3 minutes for exception handling — and the bulk of documents require no human intervention at all. The system learns from corrections, improving over time.
For NSW hospitals, the most straightforward starting point is discharge summaries or pathology reports — documents with consistent structure, high volume, and clear routing logic. These can typically go live within four weeks of an integration engagement, requiring no change to existing EPR systems.
Common Implementation Pitfall
Organisations that attempt to automate all document types in a single deployment frequently encounter accuracy problems with edge cases and lose clinician trust early. Starting with one document category — highest volume, most consistent structure — and expanding only after measurable accuracy is confirmed is the approach that consistently produces durable results.
Win 2: Smart Scheduling — 682% ROI from Demand-Driven Appointment Management
The Problem
No-show rates in NSW hospital outpatient departments run at 15–20%, and the consequences compound throughout the day. Each unfilled slot wastes specialist time that cannot be reallocated. Rostering gaps in shift-based departments result in overtime that costs the organisation more than the missed appointment. Across a department, these inefficiencies accumulate to more than 1,000 wasted hours per year — capacity that could serve actual patients.
Hospitals implementing AI scheduling report 682% ROI and 1,040 staff hours freed per department annually — achieved by predicting demand patterns and sending targeted reminders that reduce no-show rates.
The AI Solution
AI scheduling systems analyse historical appointment data, patient demographics, and seasonal demand patterns to predict no-show probability at the individual appointment level. High-risk appointments trigger automated reminder sequences — via SMS, phone, or patient portal — calibrated to patient preference and prior response rates. When cancellations do occur, the system automatically fills slots from a prioritised waitlist rather than leaving them empty.
The efficiency gains extend beyond no-shows. AI-driven demand forecasting allows rostering to be aligned with predicted patient volumes, reducing both understaffing incidents and unnecessary overtime. For NSW hospitals using Cerner or HealthOne, integration is a documented pathway — the scheduling AI reads and writes through existing system APIs, avoiding the need to replace existing platforms.
The reported 682% ROI reflects the combination of recovered appointment revenue, reduced overtime costs, and administrative time savings. An organisation recovering 1,040 staff hours per department per year has, in practical terms, added a meaningful portion of a full-time position without hiring.
Win 3: AI Triage — Reducing Emergency Department Waiting Times by 40–73%
The Problem
Emergency department intake currently accounts for 40% of total ED labour costs in many NSW facilities. The triage process — assessing patient urgency, directing to the appropriate care pathway, managing queue prioritisation — is performed manually by clinical staff who are simultaneously managing active treatment. Average waiting times of two hours or more for lower-acuity presentations are common, and the proportion of avoidable ED presentations continues to grow as GP access deteriorates.
A UK NHS study found that AI triage systems achieved a 73% reduction in waiting times by intelligently diverting 15–20% of low-risk presentations to virtual care pathways — a result now being replicated in Australian settings.
The AI Solution
AI triage systems present patients with a structured symptom assessment at the point of arrival — via a tablet, kiosk, or telehealth front door — and classify urgency against clinical decision rules. Presentations that fall below the threshold for in-person emergency care are diverted to virtual consultation or same-day GP referral, with appropriate safety netting. The 15–20% diversion rate documented in comparable deployments directly reduces queue length for genuine emergencies and frees triage nurses for higher-acuity assessment.
The waiting time reductions reported across deployments range from 40% to 73%, with the higher end coming from systems where the telehealth pathway was well-resourced and the AI had sufficient historical data to calibrate its classification model. The practical starting point for NSW hospitals is a telehealth front-door pilot targeting the most common low-acuity presentations — typically upper respiratory infections, minor musculoskeletal injuries, and medication reviews.
The 6-Phase Implementation Framework
The 6-phase model below reflects the delivery sequence used in Australian health AI engagements. The total timeframe runs 12–18 months, with contract values typically in the $1–5 million range depending on scope. The critical design principle is that no internal AI team is required — the external partner manages build, integration, compliance, and ongoing optimisation.
Phase 1: Discovery (4 Weeks)
A structured audit of clinical workflows, existing data systems (including EPR configuration), document volumes, and scheduling patterns. For Westmead or John Hunter, this typically surfaces three or four viable starting points. The output is a prioritised opportunity map with estimated implementation cost and ROI for each.
Phase 2: Data Readiness (2 Months)
Health data cannot be fed into AI systems without de-identification, compliance review, and often structural reformatting. This phase handles consent frameworks, data quality remediation, and AHPRA-compliant data governance. It is tedious work that is routinely underestimated — and the reason this phase is scoped explicitly rather than absorbed into the pilot build.
Phase 3: Pilot Build (3 Months)
The highest-priority use case — typically document automation or scheduling — is built and deployed in a controlled environment. Target metrics are set in advance. Clinical staff are involved in validation. The goal is a live system with measurable output, not a proof-of-concept that lives in a sandbox.
Phase 4: Full Rollout (4 Months)
Triage integration is added alongside the expanded rollout of Phase 3 outcomes. Change management and training are delivered to clinical teams. The system is connected to production EPR environments rather than test instances.
Phase 5: Training and Governance (Ongoing)
AHPRA-compliant AI governance modules are delivered to clinical leads. Staff are trained to interpret AI outputs, override when appropriate, and escalate edge cases. This is not a one-time event — governance is maintained as the system evolves and patient volumes change.
Phase 6: Managed Optimisation (12+ Months)
Ongoing monitoring, model retraining as new data accumulates, and performance benchmarking against the targets set in Phase 1. This phase is what converts a successful pilot into sustained organisational value — and is the phase most commonly omitted by organisations that attempt in-house delivery.
Where to Start
The most common planning mistake is treating all three wins as simultaneous targets. Organisations that attempt parallel deployment across document automation, scheduling, and triage consistently encounter integration conflicts, staff fatigue with change, and diffuse accountability. The evidence from Australian deployments points in a different direction: start with one use case, prove the result, then expand.
For most NSW health organisations, the best starting point is document automation applied to a single document category. The reasons are practical. The data requirements are modest compared to triage. The integration surface is limited. Accuracy is measurable within weeks of deployment. And the cost savings — documented at $670,000 per year in one NSW setting — are visible enough to secure executive support for the next phase.
Organisations with a more pressing scheduling problem — chronic no-shows, persistent overtime, or a waitlist management crisis — may find Smart Scheduling a stronger first deployment. The integration with Cerner or HealthOne is established, and the 682% ROI benchmark reflects results that are achievable within the first 12 months.
AI triage is the highest-complexity starting point because it touches clinical decision-making directly and requires robust safety netting. It is best approached as a Phase 4 deployment, after the organisation has developed confidence in AI system governance through a less clinically sensitive use case.
Implementation Checklist
Before engaging an external delivery partner, health organisations should work through the following readiness steps:
- Identify your highest-volume document category or your worst-performing scheduling metric
- Map the current data systems in use — EPR platform, document management, scheduling software
- Confirm existing data governance frameworks and identify any gaps against AHPRA requirements
- Nominate a clinical lead who will be the operational owner of the AI system — not a project manager
- Set a baseline measurement for the problem you are trying to solve before any AI system is deployed
- Define the minimum result that would justify expanding from pilot to full rollout
- Confirm that the delivery contract includes ongoing managed optimisation — not just implementation
Questions About Implementing AI in Healthcare?
If you're weighing up where to start or want to talk through how these applications fit your specific hospital or health network, feel free to reach out.
Get in Touch →