What This Article Covers
- When AI admin automation is and isn't worth the investment for your health organisation
- What your coordinators' workday actually looks like before and after deployment
- A realistic business case — with a calculator you can adjust to your own numbers
- How the system works in plain language, without vendor pitch or technical jargon
- What it costs, what your team needs, and how to know it's working
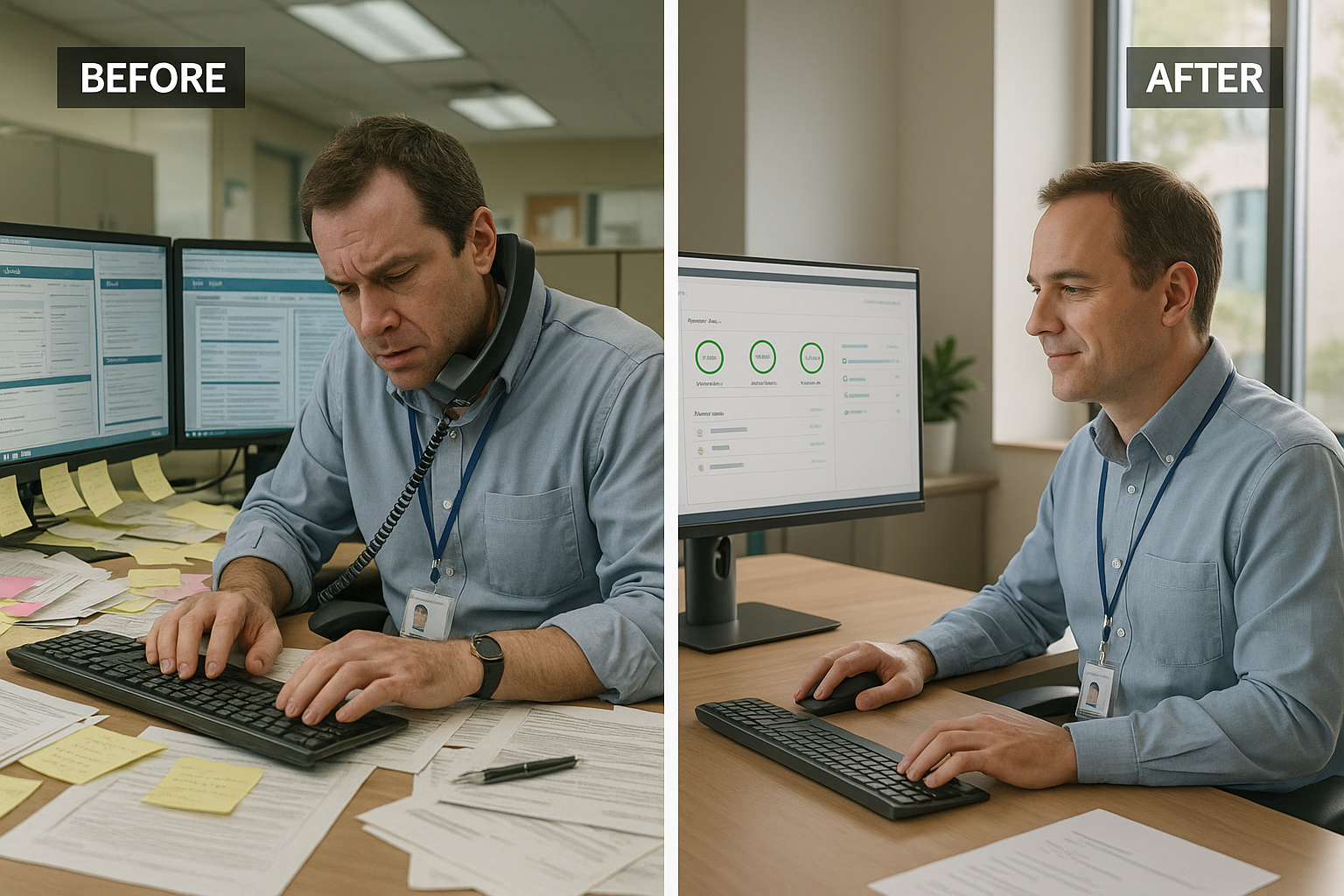
It's 9 AM on a Tuesday and your authorisation coordinator is already three cases behind. She opened the electronic health record (EHR) at 8:05, copied the clinical summary into the insurer's online portal by hand, called the payer's provider line at 8:23, waited on hold for eleven minutes, and is now re-entering the patient's date of birth because the portal timed out. One prior authorisation. Forty-seven minutes. Fourteen more to go today.
Now run that same Tuesday in a hospital that deployed AI admin automation six months ago. The system read the EHR overnight, drafted the authorisation, matched it against the insurer's criteria, and flagged two cases as likely to require additional clinical notes. The coordinator logs in at 8:05, reviews seven completed submissions in twelve minutes, adds the notes the system flagged, and has cleared her queue before the morning briefing. Same workload. Different outcome.
This article is about how that shift happens — what it takes, what it costs, and when it's not worth attempting.
1. Is This Right for Your Operation?
I'll address this upfront, because too many health organisations invest in automation before confirming the basics. The numbers look compelling in every vendor demo. The question is whether they hold at your specific site, with your specific payer mix, and your existing systems.
This works well if your organisation:
- Processes more than 200 prior authorisations or insurance submissions per week across your department
- Has an EHR system in place (Epic, Cerner, Meditech, or equivalent) with reasonably structured clinical data
- Sees an authorisation denial rate above 20% — a sign that staff are spending significant time on re-submissions and appeals
- Has admin staff spending more than 35–40% of their day on document entry and status follow-up rather than patient-facing tasks
- Operates across multiple insurance networks, each with different criteria and portals — the more payer complexity, the higher the AI return
Walk away from this idea if:
- Your clinical team has fewer than 50 staff — the fixed implementation cost rarely pays back at that scale
- Your EHR data is inconsistently structured or your records are still primarily paper-based — AI cannot extract what isn't digitised
- Your payer mix is highly unusual or dominated by a single insurer with non-standard criteria — the model's accuracy drops sharply on edge-case volumes
- Your IT team is already at capacity or has no bandwidth for a 4–6 month integration project — an underfunded deployment creates more problems than it solves
- Leadership is not prepared to enforce the new workflow — if coordinators revert to manual entry after training, you are paying for software nobody uses
Be sceptical of any vendor quoting blanket results across all hospital sizes. A 200-bed district hospital and a 1,200-bed tertiary centre have fundamentally different authorisation volumes, payer relationships, and IT infrastructure. The numbers in this article are calibrated for mid-size Australian health networks processing 300–800 authorisations per week.
2. What Changes Day-to-Day
Before: The Manual Processing Loop
A prior authorisation coordinator's day runs on copy-paste and phone queues. She opens the EHR, reads the clinical notes, identifies the relevant diagnosis codes (International Classification of Diseases, or ICD codes) and procedure codes (Current Procedural Terminology, or CPT codes), then manually transfers that information into the insurer's web portal — which is different for every payer. She calls for status updates on pending cases, tracks outcomes in a shared spreadsheet, identifies denied cases, and begins re-submission. On a busy day, she handles fifteen to twenty authorisations. Roughly 30% are denied on first submission, each requiring a second cycle of clinical review, additional documentation, and re-submission.
The shift from one insurer portal to another costs two to four minutes each time. A phone hold for status costs eight to fourteen minutes. A denied case costs an additional forty to sixty minutes of re-work. This is where the bulk of admin time disappears — not in the authorisation itself, but in the friction between systems.
After: The Review-Only Workflow
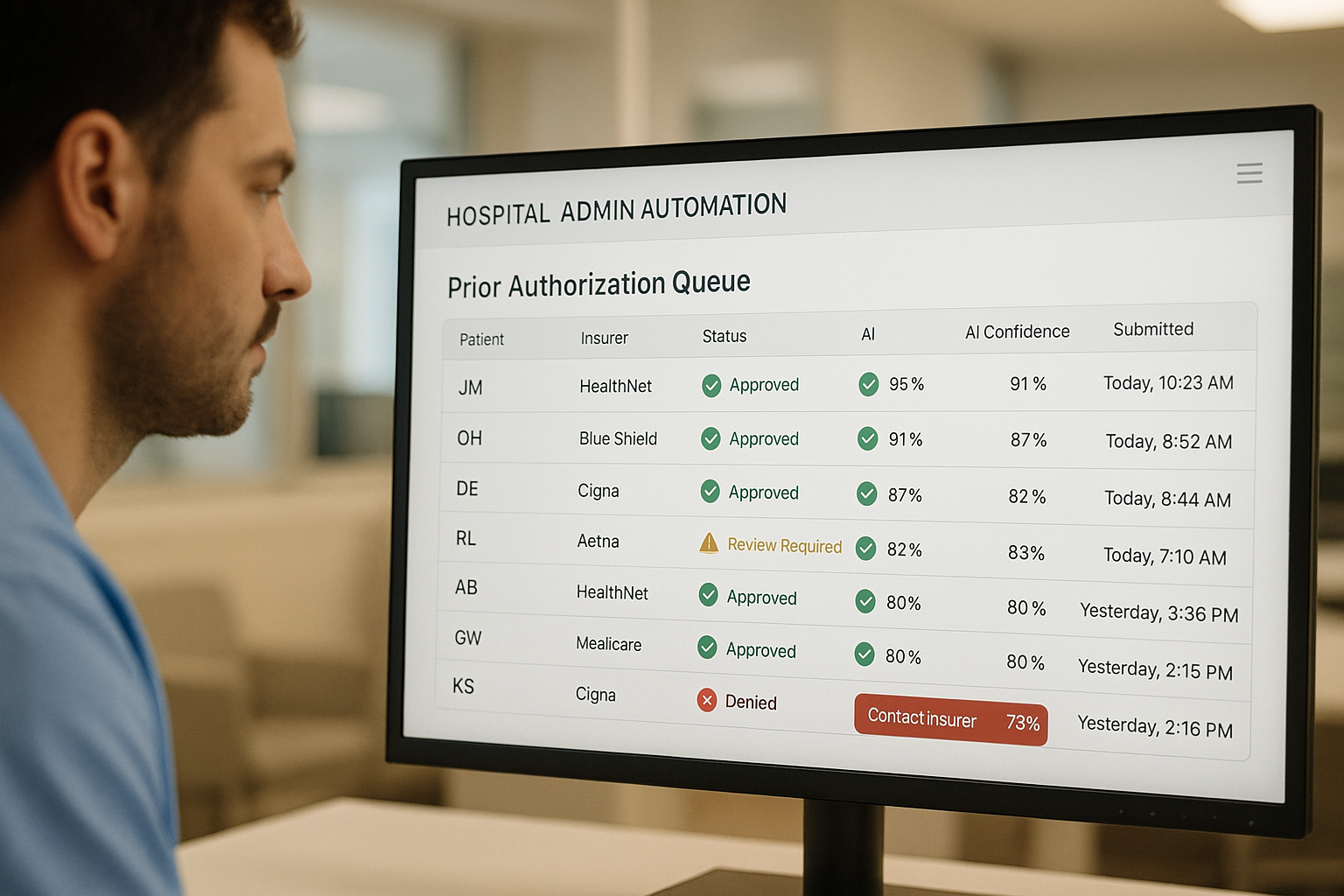
With AI admin automation in place, the coordinator arrives to a queue rather than a stack of new cases. The system has already read the overnight EHR updates, identified pending authorisations, extracted the relevant clinical data, matched each case against the insurer's current criteria, and drafted the submission. Cases the system is confident about are submitted automatically. Cases with missing information, unusual codes, or a high predicted denial risk are flagged for human review with the reason noted.
The coordinator reviews flagged cases — typically 15–25% of the total queue — adds clinical notes where needed, and approves the submissions. Average review time per flagged case: eight to twelve minutes. The clean cases: zero manual time. Status tracking is automated. Denial alerts surface in the dashboard with suggested next steps already populated.
"The shift in mindset is from processing documents to reviewing decisions. Your coordinators stop being data-entry clerks and start being clinical gatekeepers. That's a better use of their expertise — and it's what keeps them from burning out."
3. The Business Case
The number that surprises most people is not the time saving — it's the denial rate improvement. Hospitals running AI-assisted authorisation typically see first-pass approval rates rise from 68–72% to 88–93%. Each avoided denial is worth the cost of the re-submission cycle: forty to sixty minutes of coordinator time, potential patient care delays, and the administrative overhead on the clinical team asked to provide supporting documentation. At $65 per coordinator hour (fully loaded cost), a 20-percentage-point reduction in denials across 500 weekly authorisations saves approximately $338,000 per year in re-work alone — before you count the processing time reduction.
The full picture includes three categories of return: direct labour savings from faster processing, denial reduction savings from higher first-pass approval, and indirect savings from faster patient throughput when authorisations no longer delay scheduled procedures. Most Australian health networks see payback in nine to fourteen months on a full implementation.
ROI Calculator
Adjust the sliders to match your operation. Results update in real time.
Assumes 47 min average processing time reduced to 9 min per authorisation, 76% of cases handled without manual entry. Excludes denial-reduction savings, patient throughput gains, and staff retention benefits.
Authorisation Processing Hours Per Quarter — Mid-Size Health Network
Q1–Q4 2025: manual processing baseline. Q1 2026: AI deployed mid-quarter with mixed results as staff adapted. Q2–Q4 2026: full throughput at AI-assisted rate. Ramp-up quarter is expected — plan your staffing accordingly.
One important caveat on these numbers: the time saving kicks in fully only after coordinators are comfortable with the review-only workflow, typically eight to twelve weeks post-deployment. During that ramp-up period, expect processing time to improve by only 30–40% as staff build confidence in the system's outputs. Budget your ROI projections from month four, not month one.
4. How the System Works
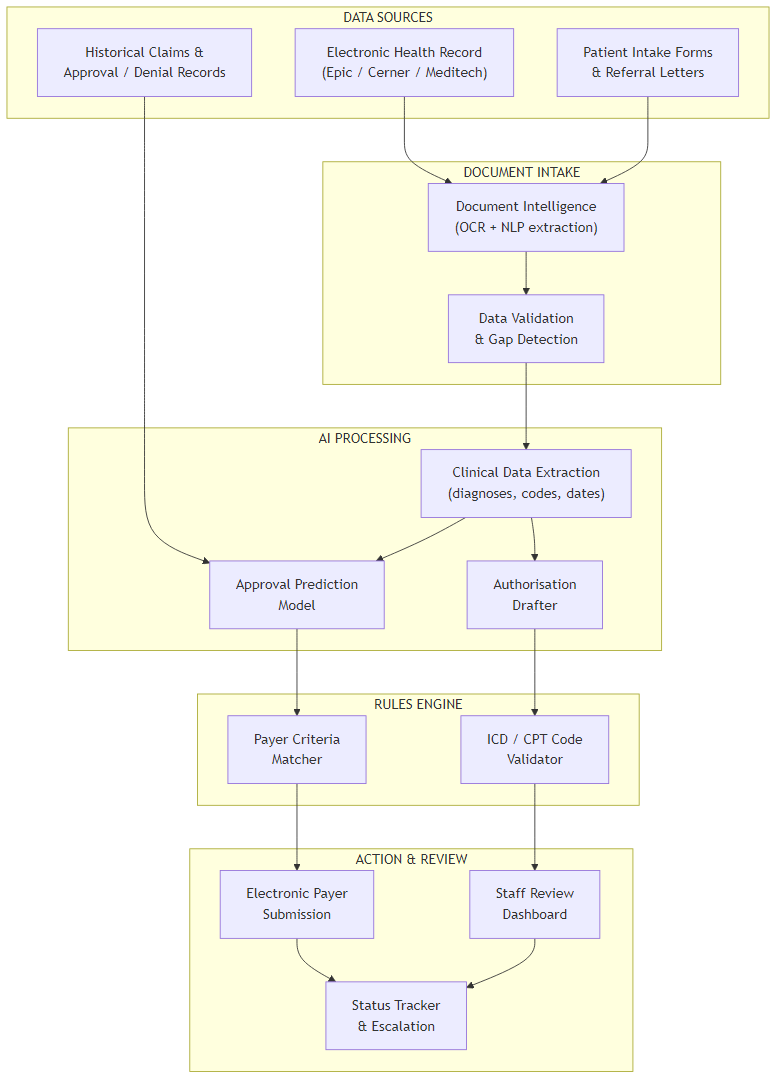
The system connects to your existing EHR and follows six stages from clinical data to submitted authorisation:
- Data Intake: The system reads the EHR overnight or on a trigger (new referral, procedure booking). It also ingests any scanned referral letters or intake forms using optical character recognition — technology that converts scanned documents into structured text your EHR cannot yet read.
- Extraction and Gap Detection: A natural language processing engine (software that reads and interprets clinical text) extracts the relevant data points — patient demographics, diagnosis codes, procedure codes, treating clinician, insurance fund, and policy number. It simultaneously checks for gaps: missing mandatory fields the insurer will require, flagging them before submission rather than after denial.
- Approval Prediction: The AI model, trained on your historical claims and approval/denial records, estimates the likelihood of approval given the extracted data and the specific insurer's current criteria. Cases predicted above 90% confidence are auto-submitted. Cases below that threshold are queued for coordinator review.
- Authorisation Drafting: For cases proceeding to submission, the system drafts the complete authorisation document, pre-populating all insurer-required fields using the extracted data. It validates ICD and CPT codes against the insurer's accepted code list, catching coding mismatches before they cause denials.
- Electronic Submission: The completed authorisation is submitted directly through the insurer's electronic portal or Application Programming Interface (API — a direct software-to-software connection that bypasses manual web portal entry entirely). No copy-paste. No portal timeout re-entry.
- Tracking and Escalation: The dashboard updates in real time as payer responses arrive. Approvals are recorded automatically. Denials surface with the denial reason pre-populated and suggested next steps — additional clinical notes, code substitutions, or escalation to a clinical reviewer — already drafted.
5. How the AI Reads Clinical Documents
Here's an analogy that's closer to the truth than most vendor explanations. Imagine a senior authorisation coordinator who has spent ten years memorising every insurer's requirements — not just the written criteria, but the patterns: which insurers approve certain procedure codes only with specific supporting diagnoses, which funds have changed their criteria in the last six months, which combinations of codes trigger an automatic review request. That institutional knowledge is the difference between a 68% first-pass approval rate and a 91% rate. The AI is building that same pattern library — but from your actual historical data rather than from memory.
Why Static Rules Don't Solve This
Most hospitals have already tried building rule-based systems — if diagnosis A then submit form B, if code X then add field Y. These break within weeks because insurer criteria change constantly: new item numbers, revised thresholds, updated clinical guidelines. A static rules engine requires a human to update it every time a payer changes their requirements.
An AI model trained on your claims history learns the current approval patterns automatically. When an insurer quietly shifts their approval criteria (as they do, regularly), the model detects the change in denial patterns and adjusts its predictions — without anyone having to rewrite a rules file. That self-correction is the core operational advantage, and it's not something a spreadsheet or a basic workflow tool can replicate.
The natural language processing component handles the clinical note extraction. Clinical notes are written by clinicians for clinicians — they use abbreviations, shorthand, non-standard structures, and medical terminology that does not map neatly to the fields an insurer requires. The NLP layer reads those notes and converts them into the structured data the authorisation requires, without a human having to translate. That translation step — often invisible to management — is where fifteen to twenty minutes per authorisation disappears in a manual workflow.
6. What It Costs
I'll give you the real numbers, including the costs that most vendor quotes omit until you are deep into contract negotiation.
| Running Cost Item | Monthly Cost (AUD) | Notes |
|---|---|---|
| AI platform SaaS licence | $2,500 – $4,500 | Per-organisation pricing; scales with monthly authorisation volume |
| EHR integration maintenance | $800 – $1,200 | Vendor or internal IT time to maintain the EHR data connection |
| Payer portal API access fees | $200 – $600 | Some insurers charge for API access; check with your top 5 payers |
| Internal IT oversight | $600 – $900 | ~0.25 FTE IT coordinator time for monitoring and updates |
| Total monthly running cost | $4,100 – $7,200 | $49,200 – $86,400 per year |
| One-Time Project Cost | Cost Range (AUD) | Notes |
|---|---|---|
| Vendor implementation and configuration | $45,000 – $85,000 | EHR connection, payer portal mapping, model training on historical data |
| EHR integration build (if custom) | $15,000 – $30,000 | Required if your EHR is not natively supported by the vendor |
| Staff training and change management | $8,000 – $15,000 | Coordinator training, workflow documentation, champion program |
| Pilot and testing phase | $5,000 – $12,000 | 8-week pilot on a single insurer network before full rollout |
| Total one-time project cost | $73,000 – $142,000 | Median for a mid-size health network: ~$95,000 |
The Number That Surprises Most Organisations
Vendor quotes almost always lead with the platform licence. What they don't lead with is the EHR integration cost — which can double the project budget if your EHR is not on their standard integration list. Before accepting any quote, ask two questions explicitly: "Is our EHR on your standard integration list?" and "Is the EHR integration build included in this quote?" If the answers are no and no, add $15,000–$30,000 to your budget before the conversation continues.
The second hidden cost is payer API access. If your top three insurers don't offer an electronic submission API — and some Australian private health funds still don't — the system will still submit via the web portal, which limits the automation and reduces the processing time saving by 30–40%.
Where Your Current Admin Spend Goes
The red slice is the primary target. AI shifts spend from manual processing and re-work to oversight and exception handling.
7. What Your Team Needs
Here's what I've seen derail otherwise sound projects: the assumption that the vendor handles everything and your team just shows up for training. That's not how it works. A successful deployment requires three internal roles — none full-time, but all present and accountable.
IT Coordinator (0.5 FTE): Owns the EHR data connection, coordinates with the vendor during integration, monitors the data feed post-deployment, and manages updates when your EHR version changes. This person does not need to understand the AI — they need to understand your EHR's data structure and have access to the integration middleware.
Clinical Champion (0.2 FTE from existing staff): A senior authorisation coordinator or clinical admin manager who understands the authorisation workflow deeply, can validate the system's outputs during the pilot, and serves as the first point of contact when staff have questions about a flagged case. This role is critical for adoption. Staff are more likely to trust a system if a respected colleague has vouched for it.
Project Sponsor (executive level): A Director of Operations or Chief Financial Officer who has approved the project, can remove blockers during implementation, and will hold the organisation accountable to the new workflow post-deployment. Without this, projects stall at the first obstacle — usually the EHR vendor's integration timeline.
On the build versus buy question: for AI admin automation in healthcare, buy. The clinical-grade accuracy requirements, payer API maintenance, and compliance obligations (particularly around the Privacy Act 1988 and the Australian Privacy Principles) make a custom build impractical for any health network without a dedicated clinical informatics team. Evaluate vendors on two criteria above all others: their EHR integration track record with your specific system, and whether their data processing agreements are compliant with Australian privacy law.
| Phase | Weeks | Key Activities | Who Leads |
|---|---|---|---|
| 1. Discovery & Scoping | 1–4 | Audit authorisation volume, payer mix, denial rates; confirm EHR compatibility; select vendor | Project Sponsor + IT Coordinator |
| 2. EHR Integration Build | 5–10 | Connect EHR data feed; map clinical fields to authorisation requirements; establish payer API connections | IT Coordinator + Vendor PM |
| 3. Model Training & Pilot | 11–18 | Train AI on 12–18 months of historical claims; run 8-week pilot on one insurer network; measure accuracy | Clinical Champion + Vendor |
| 4. Staff Training | 17–19 | Train all coordinators on review workflow; update SOPs; run supervised sessions on live cases | Clinical Champion |
| 5. Full Deployment | 20–24 | Expand to all insurer networks; move from assisted to autonomous submission for high-confidence cases | IT Coordinator + Clinical Champion |
| 6. Optimisation & Review | 25–30 | Review KPIs against targets; adjust confidence thresholds; add new payer integrations as needed | Project Sponsor + Clinical Champion |

8. How You Know It's Working
Set these five metrics as your baseline before deployment and measure them monthly. If you don't have baseline numbers, spend four weeks collecting them manually before go-live — you cannot demonstrate ROI without a before figure.
| Metric | Baseline (Typical) | 12-Month Target | How to Measure |
|---|---|---|---|
| Average processing time per authorisation | 42–52 minutes | <12 minutes | Sampled time-and-motion study; dashboard timestamps |
| First-pass approval rate | 68–72% | >88% | Monthly claims report — approvals ÷ total submissions |
| Coordinator hours per 100 authorisations | 80–90 hours | <22 hours | Payroll hours allocated to authorisation team ÷ volume |
| Denial appeal rate | 25–32% | <10% | Appeals lodged ÷ total denials received |
| Cost per authorisation processed | $38–$52 | <$14 | Total admin cost (salaries + system) ÷ monthly volume |
In practice, the right setting for most sites is to treat the 12-month target as a floor, not a ceiling. The best-performing implementations hit these numbers by month eight and then look for the next efficiency opportunity — usually automating the denial appeal drafting, which follows naturally from the same document intelligence infrastructure.
9. Where to Start
If the numbers in Section 3 are compelling and you've confirmed the basics in Section 1, here are five concrete actions to take in the next 30 days:
- Run a four-week authorisation audit. Count weekly volume, measure average processing time per case (use a one-week time-and-motion study), calculate your current denial rate, and identify your top five insurers by volume. These numbers are your baseline — without them, you cannot evaluate a vendor quote or measure post-deployment ROI.
- Pull 18 months of claims history. Work with your IT team or EHR vendor to extract a de-identified claims dataset: submission date, insurer, diagnosis codes, procedure codes, outcome (approved / denied / appealed), and final resolution. This is the data the AI model will train on — organisations that cannot produce it are not ready for this technology.
- Confirm your EHR's integration capability. Ask your EHR vendor whether they support HL7 FHIR (a standard data exchange format) or have a published API. If they do, integration is straightforward. If they don't, factor the custom integration cost into your budget before approaching any AI vendor.
- Run a vendor sandbox session on your top insurer. Before committing to any platform, ask vendors to demonstrate the system on your actual workflow — not a demo environment. Give them five real (de-identified) historical cases and ask them to show you what the system would have done with each one. Compare their predicted outcomes to your actual outcomes.
- Design an 8-week pilot scoped to one insurer network. Pick your highest-volume insurer with the most structured electronic portal. Run the AI system in parallel with your manual process for eight weeks — coordinators still process cases manually, but the system also processes them and you compare outcomes. This gives you real accuracy data before you hand over any live submissions.
Key Takeaways
- Is the opportunity real? Yes — if you process >200 authorisations per week and see denial rates above 20%, the labour saving and denial reduction together close a business case in under 14 months at most mid-size Australian health networks.
- Is it the right time? Only if your EHR data is structured, your IT team has capacity for a 4–6 month integration project, and leadership will enforce the new workflow after deployment.
- What's the realistic saving? Use the calculator above with your numbers. The median outcome for a 500-authorisation-per-week network is $380,000–$520,000 in annual labour and denial-reduction savings against a $95,000 implementation cost.
- What's the honest risk? A failed deployment costs as much as a successful one — the difference is change management. Organisations that invest in a clinical champion and enforce the review-only workflow see results. Those that treat it as a plug-and-play IT project do not.
- Where to start? Four-week audit first. No vendor conversation before you have your volume, denial rate, and claims history ready. Vendors calibrate their solutions to your numbers — if you don't have them, you're negotiating blind.
Want Practical Insights on AI in Operations?
I write about applying AI to real business problems — with honest numbers and no vendor speak. Subscribe for articles delivered twice a month.
Subscribe to Newsletter →